Making Prevention Possible
Innovative proprietary preemptive screening technologies from CDx help improve patient outcomes and reduce healthcare costs for payers.
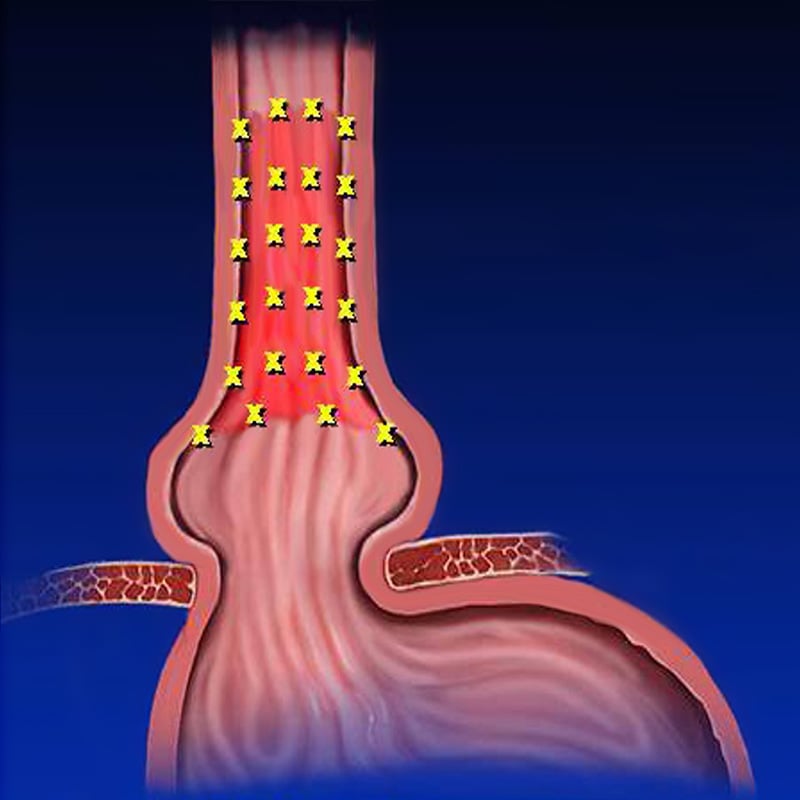
The Seattle random forceps biopsy protocol does not reliably detect Barrett’s esophagus or dysplasia, which are precursors to esophageal adenocarcinoma.
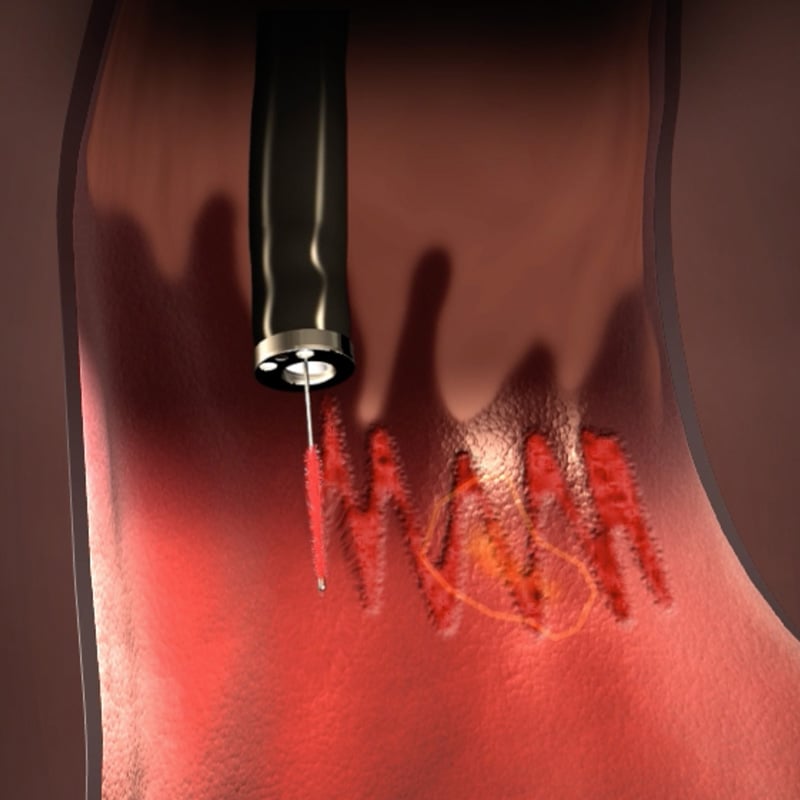
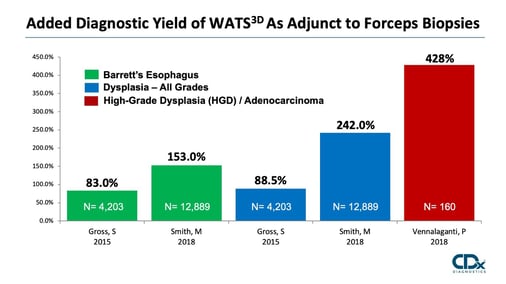
WATS3D (Wide-Area Transepithelial Tissue Sampling with computer-assisted 3D analysis), when used as an adjunct to standard biopsy sampling, has been shown to reliably detect unhealthy cells before they develop into cancer.
WATS3D is endorsed for both screening and surveillance of patients with suspected or known Barrett's esophagus , as an adjunct to routine biopsies, in the recently published Guidelines of the American Society for Gastrointestinal Endoscopy (ASGE).
“In patients with known or suspected BE, we suggest using WATS3D in addition to WLE with Seattle protocol biopsy sampling compared with WLE with Seattle protocol biopsy sampling alone”
*ASGE guideline on Barrett’s (GI Endosc 90(3) 2019 page 351)
EAC is preventable if detected and treated early. WATS3D has demonstrated the ability to improve patient outcomes by having a direct impact on the clinical management in 97% of patients diagnosed with BE, LGD or HGD.
Clinical utility of wide-area transepithelial sampling with three-dimensional computer-assisted analysis (WATS3D) in identifying Barrett’s esophagus and associated neoplasia.
Vivek Kaul, Seth Gross, F Scott Corbett, Zubair Malik, Michael S Smith, Christina Tofani, Anthony Infantolino
Diseases of the Esophagus, July, 01 2020
https://doi.org/10.1093/dote/doaa069
More than half of the US population is now over the age of 50, an age that is at increased risk for developing esophageal adenocarcinoma. Detecting dysplasia early and treating, it has the potential to reduce the incidence of this deadly disease. The addition of WATS3D per 1,000 patients results in approximately 3 fewer cancers and 3 fewer cancer-related deaths.
Wide Area Transepithelial Sampling with Computer-Assisted Analysis (WATS3D) Is Cost-Effective in Barrett’s Esophagus. Screening. Singer ME. Gross S, Kaul V, Smith MS. 449. Digestive Diseases and Sciences: June 23, 2020.
https://doi.org/10.1007/s10620-020-06412-1
WATS3D when used adjunctively to standard forceps biopsy is more cost-effective for Barrett's esophagus screening compared to forceps biopsy alone. Screening with WATS3D costs an additional $1,219 and produced an additional 0.017 QALYs, for an ICER of $71,395/QALY.
Wide Area Transepithelial Sampling with Computer-Assisted Analysis (WATS3D) Is Cost-Effective in Barrett’s Esophagus. Screening. Singer ME. Gross S, Kaul V, Smith MS. Digestive Diseases and Sciences: June 23, 2020.
https://doi.org/10.1007/s10620-020-06412-1
For more information about our products and services or general questions, we are here to help.
